
{kind=link}
So, you’ve been told you’ve broken a bone. Is this the same as a fracture? How long will it take to resolve? Do I need a sling or a brace? What should I be doing to ensure the bone heals properly? There are often a lot of questions, in what can be a stressful injury to be diagnosed with.
As I’m writing this I’m wearing a plaster around my arm eight weeks into a hand fracture. Ha ha. The irony.
But like you, I was overwhelmed with questions and concerns initially, so I’ll try and flesh these out for you.
What is a bone fracture?
To put it simply, a fracture is a break or a crack in the bone. Unfortunately, there are quite a few terms used to differentiate between different types of fractures that you may be reading through on your scan report.
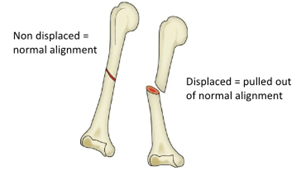
Displaced vs undisplaced: A displaced fracture often occurs where the bone breaks in two or more places and moves out if its normal alignment. An undisplaced fracture means that the bone breaks but doesn’t move out if it’s normal alignment. In theory, if you immobilise and stop moving your undisplaced fracture for long enough, it will return to its normal alignment.
Open vs closed: An open fracture breaks through the surface of the skin, a closed fracture doesn’t.
Stress fracture: Tiny cracks in the bone caused by repetitive stress or force over time.
Intra articular vs extra articular: An intra articular fracture has the fracture line extended into the joint. An extra articular fracture has a fracture line that doesn’t extend into the joint.
There are plenty of other terms used to describe fractures, but these are the basics.
How do I get a fracture diagnosed?
Most of the time, an X-Ray is the first point of call to diagnose a fracture. It’s cheap, it’s easy and most of the time they give you enough information required to diagnose a fracture.
However…
Some fractures can be missed on X-Ray. Often this depends on the bones involved, as some of the smaller fractures in a hand or foot can be missed on the X-Ray. Significant swelling can also make it more difficult to attain an accurate X-Ray. As a basic guideline:
– If your pain isn’t improving
– If you had significant swelling during the initial injury
– If you have night pain (when your bodies’ natural anti inflammatories are at their lowest)
– No fracture was shown on X-Ray
Then it would be a good idea to consult with a Physiotherapist on a management plan and what sort of other imaging can be used to diagnose a suspected fracture. A CT or MRI offer higher levels of detail and will pick up fractures that can be missed on a standard X-Ray.
I’ve been diagnosed with a fracture, what should I do?
Once again, consulting with a physiotherapist is a great start as different fracture types require different treatment. In terms of your management, the majority of fractures will start off with some form of immobilisation, a period of time where it is required to reduce or eliminate motion, so that the fracture can heal.
Going back to our definitions from before, if a displaced fracture is left untreated in its unaligned position, the fracture will heal in a position that doesn’t allow for full movement or movement with reduced joint surface contact. This causes that part of the joint to wear out quicker, with the potential to increase risk of arthritis.

Should I get surgery if my fracture is displaced?
Most of the time, a consult with an orthopaedic surgeon with a referral from your Physiotherapist is worthwhile. Depending on your age, goals and type of fracture, a decision will be made on whether you need surgery or not.
Most surgeries for a displaced fracture will require reduction, a process where the bones are realigned so that they heal in an ideal position. This will either require special instruments that help separate the bones so the fracture can be adjusted, or a cut is made through the skin to fixate the fracture with plates and screws.
There is normally still a period of immobilisation after surgery to ensure that the modified bone is protected.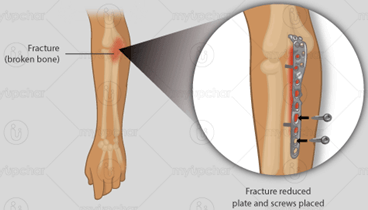
Is there anything I should be doing while I’m waiting for my fracture to heal?
Absolutely, here’s a few productive things you can do while you’re immobilised to give you the best chance of a successful recovery.
Diet
Sufficient quantities of calcium and vitamin D are always a good start. But also sufficient amounts of vitamin C, lysine and proline amino acids, and other micronutrients that support the structure of collagen. These nutrients help form collagen, shown to increase bone mineral density.
Cross Education
A phenomenon where training one side of the body results in an increased strength of the OPPOSITE side of the body. Basically, your brain becomes more efficient at coordinating and performing strength based movements, and can begin to use these gains on the affected limb once you’re out of your plaster or brace.
Staying Active
Particularly if you’re returning to sport, continuing to exercise within your capabilities will ensure you have less work to do once your fracture is healed. I.e. If your upper body is affected, train lower body. And vice versa. Physios can be very creative in administering this!
So, after I have surgery and I’m out of my brace or sling, I’ll be good to go right?
Not quite, depending on what you’re getting back to its very likely you’ll need at least some rehab. While a joint is immobilised it’s very normal for the muscles around that area to weaken and become stiff on account of not being able to stretch while in a cast or brace.
More demanding activities, such as contact sport would require a more extensive rehab ensuring that the affected joint and fracture site is able to withstand force and impact to avoid re injury.
I’ve had a fracture and been told I’m osteoporotic, do I need to wrap myself in cotton wool and avoid exercise forever?
Absolutely not! Exercise is your biggest tool in terms of trying to improve your bone health. While resistance training can help increase muscle strength to support bones, most of the gains actually come from exposing the bone to load. Walking, jumping, hopping and skipping are all great ways to load up your bones so that they get stronger and less likely to fracture in the future.
So, there you have it, hopefully your outlook on your recovery from a fracture is trending in the right direction. Some of the key things that have helped me dealing with my fracture are:
– Focusing on what you can do, not on what you can’t.
– Having a really clear view on your healing timelines, ticking off your weeks on a calendar is a great way to remind yourself of the progress you’re making.
– Having a plan of what you need to after you’re out of your brace or cast to get back to what you want to do.
If you’re currently dealing with a fracture, consulting with a Physiotherapist for a plan of attack should be your first point of call. Unfortunately, and fortunately at Pathways, most of us have had first hand experience dealing with fractures so we will definitely be able to help!
Want more advice from one of our skilled Physiotherapists on how to manage your fracture? Book Online HERE.